Leqembi infusions




Hello. I'm new to the group. My husband was recently diagnosed with MCI due to AD, 66 yo. + APOE 4. Needless to say, we are devastated. He's had mild memory loss for about 6 months. Tried aricept but had terrible GI symptoms. He's been tolerating Namenda. I haven't noticed must improvement with his ST memory. However, Leqembi and Kisunla infusions have been offered. I've done alot of research and it appears that only about 9 months of improved memory has been gained. I've read numerous posts here about these infusions and while it seems that those who are using the infusions are doing well, there doesn't seem to be any posts as to whether it has helped with ST or LT memory gain. My husband is reluctant to do the infusions due to the potential of ARIA. Thank you for your feedback.
Comments
-
0
-
I just had my 33rd Leqembi infusion. Here is one data point: I had the Montreal Cognitive Assessment (MoCA) performed twice: a few months before starting on Leqembi and after about 10 months on Leqembi. I scored the same on both tests.
I'd suggest you aren't quite reading the study results correctly. Cognitive decline is a common characteristic of AD. In the respective Phase 3 clinical trials for Leqembi & Kisunla, they both slowed the cognitive decline by about the same percentage. Some folks have converted this percent slowing of cognitive decline into time, as that is seemingly easier for us common folk to understand.
Thus, in general, neither drug "helps with ST or LT memory gain." Rather, both drugs help slow ST/LT memory loss.
There is one exception. In the Phase 3 trials for both drugs, they did a subgroup analyses for those with no/low levels of tau in their brains. As a reminder, the two hallmarks of AD are amyloid plaques which exist outside of neurons and tau tangles which are inside neurons. It is the tau tangles which drive the cognitive decline associated with AD. Unfortunately, no anti-tau drugs are currently available (some are undergoing clinical trials right now). The two drugs that have been approved by the FDA (Leqembi & Kisunla), are anti-amyloid drugs.
Back to the no/low tau groups. For this subset, the drugs stopped cognitive decline in a significant fraction of this group, and a small fraction in this group actually did experience a slight improvement in cognition during the clinical trial.
Yes, ARIA is a concern with these drugs. I was well aware of the risk. Both of my parents had dementia. My Dad died quickly from cancer, but my Mom lingered on while AD slowly robbed her of all of her memories.
Thus, I was very aware of what it was like to experience this disease, so for me it was a simple decision to start on Leqembi (that was the only drug available at the time). I was also considering joining a clinical trial with an anti-amyloid drug and an ant-tau trug. But that trial was delayed, so I started on Leqembi.
I respect that others may make a different choice.8 -
Thank you so much for your informative discussion. I recently went to my first appointment at Barrows Neurological where I live. That appointment was scheduled a year ago. I am tentatively excited about BNs approach and they appear to have a pretty good score on my TGAF meter I carry in my purse. Lol. They scheduled me for both an MRI and PET scan. Looking for forward to hear what they have to say after being with a neurologist for three years since I was diagnosed that scored really really high on the IDGAF about you meter.
0 -
Thanks so much for your response. Glad to hear you're maintaining cognitive function and tolerating the infusions. The MOCA comparative result was a good example for me to grasp. My husband's MOCA was 24/30, his pTau was .33 (range max .15) and "significant" amyloid plaque on PET scan. What is your age? Again, much appreciate your response.
0 -
I'm 64.7 years old (I turn 65 in January 2026).
1 -
What is the centiloid value most saw when diagnosed? My DH is in the gray area at 24 (age 64) right now. One doctor wanted him to wait for 2 years before being tested again - that was a hard NO from us. Next beter doctor said 6 months; try infusion; and PET again to see where he is in 6 mns using 30 as a positive value.
0 -
Did you try the infusions? What about the fog?
0 -
How many people out there would decide to get the infusions who are past 80 yrs. old or older???? AND are in the mild stage of Alzheimerl's? I am reconsidering the infusions after all the research, etc. I am now thinking " No " to the infusions that are available to me. Opinions??
1 -
It is a free country, so if you are fine with "letting nature take its course" with Alzheimer's, that is your perogative.
For many decisions in my life, I tend to compare risk versus reward. So for me, it was a nobrainer decision to start on anti-amyloid therapy. The risks were non-trivial, as ARIA (brain bleeding / swelling) is not a minor concern. However, I found that the potential rewards, especially for those with mild AD, are huge, by maintaining good cognition levels for a longer period of time. So from my perspective, the reward far outweighted the risks. But again, this is a free country, and I respect that others may decide they dangers of the drugs are worse than the disease.
I don't see that chronological age has much to do with the decision. The Phase 3 trial for Kisunla included people aged 60-85, in the Leqembi trial people were 50-90. People develop AD over a wide age range, and the anti-amyloid drugs were shown to be effective regardless of age.0 -
Thank you for sharing..
0 -
thank you lbc83 or sharing your experience. it is very enlightening. i have MCI and i was just diagnosed with ad after a positive tau test and a pet scan showing amyloid build up. i talked with my neurologist and he was recommending kisunla infusions for 12 months. im thinking that it might be better to go with Leqembi because of the lower chance of aria and also with the injectable option. anyone have knowledge and/or opinions on this.
thanks frank
1 -
The subcutaneous injection option for Leqembi is currently only approved by the FDA for "maintenance dosing". This term refers to completing the initial 18 month Leqembi bi-weekly infusion protocol. After that, Eisai (the company primarily responsible for Leqembi) recommended switching to infusions every four week for "maintenance dosing". Now, with FDA approval of the subcutaneous version of Leqembi for maintenance dosing, patients have a two options after completing the initial 18 month period of bi-weekly infusions: continue with infusions every 4 weeks (note the change in frequency), or switch to a weekly subcutaneous injection.
The Leqembi vs Kisunla tradeoff can get complicated. At a high level, you are comparing bi-weekly infusions for Leqembi with infusions every four weeks for Kisunla. Regarding treatment duration, we just covered the 18-month recommended length for Leqembi. In the phase 3 trial for Kisunla, participants were taken off the drug if amyloid PET scans showed amyloid plaque clearance. As the sole purpose of Kisunla is to remove amyloid plaque, it doesn't make much sense to continue treatment after all of the plaque is gone. Specifically, in the Kisunla Phase 3 trial, 17% of those taking Kisunla stopped taking the active drug at 6 months, 47% at 12 months, and 69% at 18 months. The concept of stopping Kisunla treatment after amyloid clearance seems somewhat controversial, with some Doctors recommending continuing treatment. Then there is the practical question of how one determines the amyloid level, to figure out if treatment can be terminated. Repeat lumbar punctures or amyloid PET scans are costly (and the former not exactly a joyful experience). Some of the new blood tests to check for amyloid might help solve this problem at some point in the future.
Eisai likes to note that Leqembi is "dual-acting", as it removes both amyloid plaque and amyloid protofibrils. The latter can damage neurons which is presumably bad for cognition. So one rationale for continuing with Leqembi dosing after 18 months is to continue to remove amyloid protofibrils (side note: Kisunla does not address amyloid protofibrils).
You have to be careful when comparing Kisunla & Leqembi ARIA rates. Comparing the Phase 3 trial data for Kisunla & Leqembi, Leqembi did have lower ARIA rates. However, since the Phase 3 trial for Kisunla, Eli Lilly (drug company responsible for Kisunla) has gotten FDA approval for a revised dosing strategy. Originally, dosing for Kisunla started with two vials of Kisunla for doses #1-#3, doubling the dosing to four vials of Kisunla for infusion #4 and all subsequent infusions. A brilliant person at Eli Lilly figured out that if you shift one vial from infusion #2 to infusion #4 (so you have one vial for infusion #1, two vials for infusion #2, three vials for infusion #3, and four vials for infusion #4 and all subsequent infusions), then this might reduce ARIA rates. Sure enough, in a trial, the ARIA rates for Kisunla improved greatly. Leqembi still has a slightly lower ARIA rate, but the difference in ARIA rates between Kisunla & Leqembi are now much smaller. Much of what you might read on the web could be comparing the old Kisunla ARIA rates with Leqembi.
In terms of slowing cognitive decline associated with AD (perhaps the whole point of taking one of these drugs), using a the same measure for cognitive decline (specifically the Clinical Dementia Rating - Sum of Boxes, which is a comprehsive test assessing memory, time/place orientation, judgement / problem solving, community affairs, home & hobbies, & personal care), in the Phase 3 trial, Kisunla slowed cognitive decline by 29% compared to 27% slowing for Leqembi. A bigger number is better (more braking of cognitive decline), so Kisunla was slightly better at slowing cognitive decline compared with Leqembi. This teeny-tiny difference would perhaps not be noticable if you could somehow start on Leqembi for a year, take a cognitive test, then Quantum-Leap back in time and start on Kisunla instead for a year, then take another cognitive test and compare results.3 -
Thank you so much for this info lbc83. Your knowledge is impressive.. I did not realize the injector was for maintenance and that the kisunla risk had changed. I'm now thinking the kisunla has the edge due to once monthly infusion and slightly greater effectiveness.
Do you know anything about the tau tangles and their effects on the brain? I understand the current meds do not effect them and they continue to kill brain cells. I had a tau blood test through care access that showed elevated tau levels so I'm curious to know more
1 -
Unfortunately, there is much confusion over tau. You are correct, tau tangles seem to be a major contributor to the cognitive decline associated with Alzheimer's. At a high level, the difference between amyloid plaque and tau tangles is simple: as in real estate, the key is location, location, location: amyloid plaque exists outside of neurons, while tau tangles exist inside neurons.
With regards to the effects of the current medications, below is an illustration from an Eisai presentation (the drug company responsible for Leqembi). The red line is showing amyloid-ß plaque, the blue line tau tangles. The graphic shows what happens when this person starts on Leqembi at a specific point in their AD journey, when amyloid plaque and tau tangles are high but not yet at their maximum levels. As you would expect, following treatment with Leqembi, the red line is showing the reduction in amyloid plaque. The dotted red line shows how amyloid plaque levels might have increased had the person not started on Leqembi.
Similar story for tau. Leqembi (and presumably Kisunla) slows down the accumulation of tau tangles, but does not completely stop tau. Thus, the solid blue line bends downward slightly, compared with the dashed blue line (what tau would have looked like without starting on the anti-amyloid drug).
Then finally we get to cognitive decline. The dashed green line is showing the cognitive decline curve without treatment. There is region color coded in green, showing "high risk" and "low risk" people for cognitive decline. For both groups, taking Leqembi (again this presumably also applies to Kisunla) reduces the cognitive decline. But unlike the amyloid plaque and tau, the change in cognition differs between "high risk" and "low risk" people, with everybody else somewhere in the green region between these two limits. I haven't seen any materials from Eisai elaborating on how any of us might figure out if we are "high risk" or "low risk" people.
You mentioned your blood test included tau levels. That is another whole can of worms, with confusing terminology. Generally speaking the tau that is measured in the currently available blood tests is used as a biomarker indicator for amyloid plaque, not for tau tangles. For example, a common blood-based biomaker is called ptau-181, which stands for Phosphorylated tau strand #181. Studies have shown this correlates very well with amyloid plaque levels. But ptau-181 is not a biomarker for tau tangles. As I understand it, blood-based biomarker testing has yet gotten to the point of being able to detect tau tangles. There are studies that have shown that something called MTBR tau when measured in the blood can accurately correlate with tau tangles. But as I understand it, none of the AD blood tests that are commercially available today detect MTBR tau.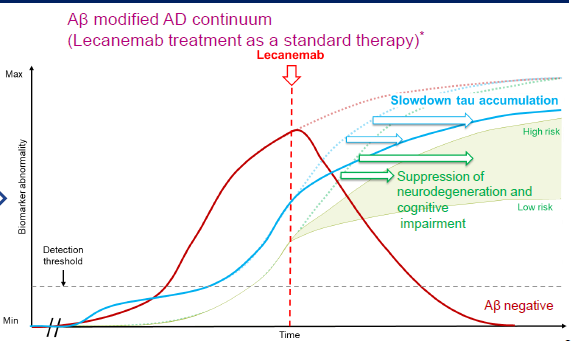 1
1 -
thank you so much for this info lbc83. i'm not sure i fully understand it yet but you cleared up my misunderstanding on the tau tests. ill have to do more reading.
3 -
I would ask for bloodwork to be done to see if you have the APOE4 gene. It is my understanding if that is the case and that gene is present it is best to go with Lequembi. I may be incorrect but I was told that . My husband had one APOE4 gene and he is taking Lequmbi.
0 -
I have one APOE4 gene and I'm also taking Leqembi. However, that is because my first infusion was in June 2024 and Leqembi was the only option.
It is difficult to compare ARIA rates between Leqembi & Kisunla simply because the Kisunla dosing strategy has changed. If you haven't been following the details, Kisunla was originally approved by the FDA with a dosing strategy of 2 vials for each of the first two infusions, then 4 vials of Kisunla for all subsequent doses. This resulted in higher ARIA rates for Kisunla compared with Leqembi. Some brilliant person at Eli Lilly suggested moving just one vial in the infusion sequence: take a single vial from the first Kisunla infusion and move it to infusion #3. This results in a very simple Kisunla dosing strategy: one vial for infusion #1, two vials for infusion #2, three vials for infusion #3, and four vials for infusion #4 and all subsequent infusions. A trial with this simple dosing change showed a reduction in ARIA rates for Kisunla. The only comparison I've seen comparing ARIA rates between Leqembi and Kisunla with the new dosing strategy still shows reduced ARIA rate with Leqembi, but the size of the difference in ARIA rates between the two drugs is much smaller. Furthermore, this new assessment was silent on the impact of APOE4 type with the ARIA rates using the new Kisunla dosing strategy.
So I don't know that there should be a general rule that if you have an APOE4 gene you should use Leqembi. There is an ARIA risk with both drugs. Kisunla has the benefit of a less frequent infusion rate (once every four weeks vs every two weeks for Leqembi). If your primary interst is in clearing out your amyloid quickly and then being done with infusions, then Kisunla seems the obvious choice as the recommendation is to stop treatments after amyloid clearance. If you prefer the "dual-acting" nature of Leqembi, so-named as Leqembi removes amyloid protofibrils as well as amyloid plaque, then you would clearly go with Leqembi and switch to maintenance dosing after 18 months of bi-weekly infusions, perhaps using the new IQLIK subcutaneous injections for maintenance dosing (which is what I hopeto do early in 2026).1 -
Hello LBC83 - checking in to see how you're doing on the leqembi infusions. My husband has considered the infusions but is unsure which one to do (Leqembi or Kisunla). Any side effects? Positive or negative outcomes thusfar? ETC…. thank you much!
1 -
0
-
Hi, I'm taking my 19th infusion of Lequimbi this week. All good so far, no complaints about Lequimbi
3 -
I have Leqembi infusion #41 tomorrow. This will be my first "maintenance dose" of Leqembi (i.e. I've completed the 18 month treatment period with bi-weekly infusions, now switching to maintenance infusions every 4 weeks). I hope to switch soon to the new IQLIK subcutaneous dosing (you administer the weekly shot yourself at home).
I have had zero side effects from the infusions.
A common question about "positive outcomes" is along the lines of "have I noticed a slowing of cognitive decline". I always find that a very difficult question to answer. I'm an Engineer by training. To answer properly, I would first need to estimate what my cognitive decline what might have been like without treatment, then compare that with my cognitive decline with Leqembi treatments. How would anybody figure out how their congition would have declined without treatment? That seems an unanswerable question. It then follows that it is rather difficult to estimate the "treatment effect" if one has no idea of what the "untreated" effect would be.
By one measure my cognition has not changed since before starting on Leqembi. I took the Montreal Cognitive Assessment (MoCA) about 5 months prior to starting on Leqembi, and then again after about 10 months of Leqembi treatments. I scored the same on both tests. I take that as a success with Leqembi.
In terms of a comparison between Kisunla & Leqembi, they both excel at removing amyloid plaque from your brain. The nice aspect of Kisunla is that treatments are every 4 weeks, versus every 2 weeks for Leqembi (that can be a big deal if you have a long drive for infusions). But that comes with a price - Kisunla has higher ARIA rates (i.e. brain swelling / bleeding) compard with Leqembi.
An often overlooked difference between the two is what happens after amyloid clearance. With Kisunla, the sole purpose of the drug is to remove amyloid plaque. Hence, people taking Kisunla stop treatments after there is evidence that your amyloid plaque levels are back to normal (i.e. a PET scan, or a lumbar puncture, or perhaps one of the new blood tests to measure amyloid plaque levels). Leqembi is different in this respect - Leqembi removes both amyloid plaque and amyloid protofibrils (smaller amyloid fibers that have not yet formed into balls of plaque). Eisai (the drug company primarily responsible for Leqembi) likes to note in their press releases about Leqembi that this "dual-acting" nature of Leqembi sets the drug apart from Kisunla. Eisai notes that amyloid protofibrils are also damaging to neurons, and amyloid protofibrils keep getting formed in your brain even after amyloid plaque is removed. Hence the Leqembi "maintenance dosing" after amyloid clearance. I recently had a blood test which showed I no longer have high levels of amyloid plaque (i.e. I'm "amyloid clear"). However, due to the nasty amyloid protofibrils that keep getting formed in my brain, I'm going to continue on with Leqembi maintenance dosing, to continue clearing out the newly formed amyloid protofibrils. Will this make a hill of beans of a difference in my progression of AD?? Who knows. Nobody has conducted a trial, taking 1,000 people who were on Leqembi and having 500 continue on with maintenance dosing and the other 500 stop treatment. Then wait a couple of years to see how the two groups perform in terms of cognitive decline. I presume nobody ever will conduct such a trial - who would want to volunteer to risk getting a placebo for a couple of years when they could be receiving a maintenance dosing of Leqembi?!? So I don't know if we will ever know how effective Leqembi maintenance dosing really is. This reminds me of gambling in Las Vegas, in this case you are wagering your cognitive decline (or a possible strategy to continue to minimize cognitive decline).2 -
Thank you so much for sharing this valuable information / experience. I declined the infusions after 6 months of stress waiting for insurance approval. I am 80, and based a part of that decision on my age & the fact that I'm still not seeing any real signs of progression as I am still taking care of ALL my finances, etc. as before. It seems I would be about 83 by the time I finish the infusions. No one in my family of 7 sibblings have lived to that age. So many unanswered questions in my opinion. I would be gone before any long term info is available of the success, long term advantage or lack thereof.
0 -
0
-
I'm 67, and on Humana medicare advantage Infusion meds including Lequimbi, are covered under part B. Furthermore, I've applied for Eiasi's patient copay assistance program, bringing my copay to $0. Info on the Lequebmi website- see if you're eligible.
on the
1 -
I'm also past 80 and have made the same decision as you, From what I know that benefits of available infusions in terms of slowing AD progression are modest, and the risks are not trivial. I'll continue to follow the discussion for a couple of reasons. First, there is always new information from continued experience with the infusions. And secondly, the process of staying informed and considering whether advancements in treatment indicate a reconsideration of my decision I've made is probably a good brain exercise. I do recognize that time for reconsidering my decision about treatment is not unlimited, i.e. since AD is progressive with the passage of time I may no longer be a candidate for treatments I have now rejected.
1 -
I have one APOE 4 and have been receiving Leqembi for several months. I get regular MRIs to check for ARIA/brain swelling or bleeds. SO far all is well…and I have sense little if any decline in my cognitive skills…which I credit in part to my Leqembi injections. I wish you well on this journey. Keep us posted.
0 -
I would have to agree that Leqembi appears to "lifted the fog" that I felt I lived in for about two plus years. I feel more clarity in my thought processing. It has not increased my memory forming capabilities but has allowed me to pull up the day to day short/mid term memory capabilities that allow you to get thru day to day living more easily and slowed my decline. OBTW... I have had only 11 Leqembi infusions so far.
0 -
did you have any side effects? also how long before you saw any changes? My sister had her first infusion this week and it almost seems worse
0 -
Regarding side effects, I had, and continue to have mild loose stool . A little annoying but not a big deal. I have a dramatic lack of appetite, which is kinda helpful since I am a bit overweight 😊. I have taken 11 infusions. I think I really started to feel a difference maybe around the fifth or sixth?? What I have most noticed, and close friends have commented, is increased mental clarity. For over two years since diagnosis I have felt like I was living in a mental cloud. The Leqembi appears to have lifted that cloud and I really feel mental clarity I have not felt in a long time. I don't lose track of what I was saying mid sentence anymore, or rarely. My memory still sucks big time. I have been able to retrieve long term memories more easily than prior to Leqembi. Short term memory is a bit better but I don't know if that is due to the increased clarity or if it is fact better. Hope this helps. Please reach out if you have any follow-up questions. GE
1










Commonly Used Abbreviations
DH = Dear Husband
DW= Dear Wife, Darling Wife
LO = Loved One
ES = Early Stage
EO = Early Onset
FTD = Frontotemporal Dementia
VD = Vascular Dementia
MC = Memory Care
AL = Assisted Living
POA = Power of Attorney
Read more
Categories
- All Categories
- 626 Living With Alzheimer's or Dementia
- 343 I Am Living With Alzheimer's or Other Dementia
- 283 I Am Living With Younger Onset Alzheimer's
- 17.6K Supporting Someone Living with Dementia
- 5.7K I Am a Caregiver (General Topics)
- 8.6K Caring For a Spouse or Partner
- 2.9K Caring for a Parent
- 223 Caring Long Distance
- 172 Supporting Those Who Have Lost Someone
- 12 Discusiones en Español
- 1 Vivir con Alzheimer u Otra Demencia
- 1 Vivo con Alzheimer u Otra Demencia
- Vivo con Alzheimer de Inicio Más Joven
- 11 Prestación de Cuidado
- 2 Soy Cuidador (Temas Generales)
- 8 Cuidar de un Padre
- 23 ALZConnected Resources
- View Discussions For People Living with Dementia
- View Discussions for Caregivers
- Discusiones en Español
- Browse All Discussions
- Dementia Resources
- 8 Account Assistance
- 15 Help